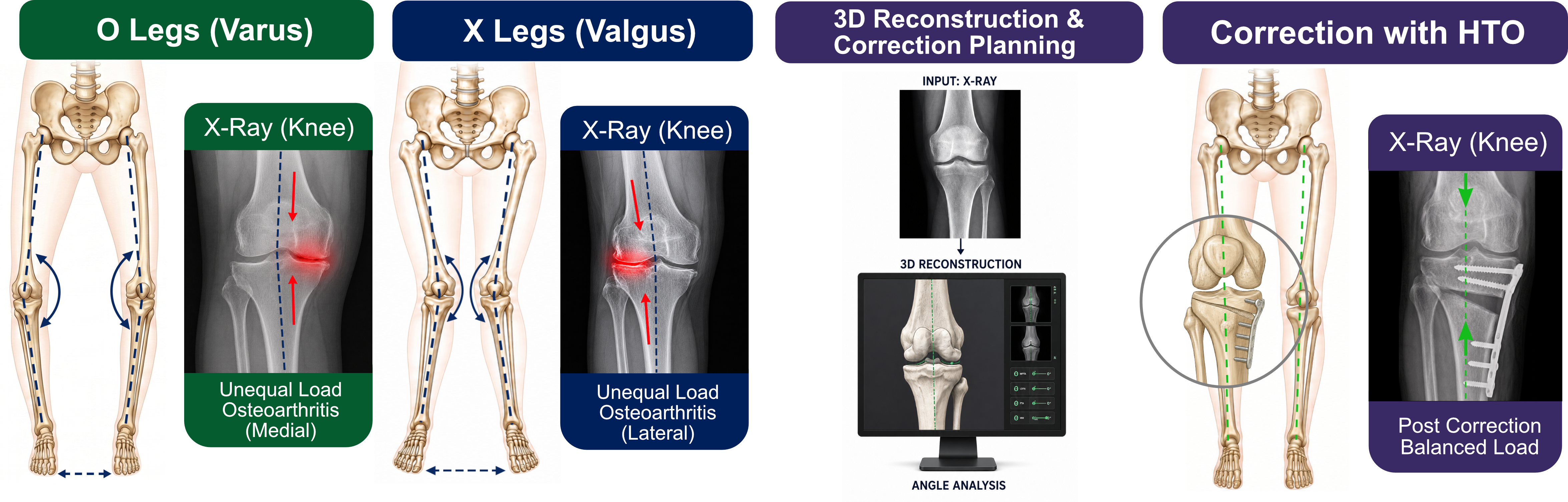
Knee osteoarthritis is a common degenerative disease that can lead to pain and reduced mobility. High Tibial Osteotomy (HTO) is a joint-preserving surgical procedure used to treat this condition by surgically correcting the leg axis. The tibial bone is cut and realigned in order to relieve load from the affected part of the knee. Currently, HTO planning is mainly based on 2D X-ray images in the coronal plane, which lack information about the third spatial dimension (sagittal and axial planes) and do not capture individual biomechanical dynamics. To address these limitations, the HTO+ project aims to improve the surgical planning by incorporating more comprehensive and patient-specific information beyond conventional 2D methods.
Goals
The project is intended to improve HTO by considering a patient-specific 3D anatomy and incorporating individualized kinetic parameters to determine the correction angle. More specifically, the goal is to generate a 3D reconstruction of the anatomy from a 2D X-ray to enable surgical planning in all three dimensions. This reconstructed 3D anatomy is then used to determine the correction angle and define the cutting plane. Based on this planning, individualized cutting templates can be generated. In addition, the project investigates whether these patient-specific templates can be automatically produced using 3D printing technologies. To correctly determine the optimal leg correction angle and therefore the 3D plane, we will need first to investigate the different characteristics angles via a lower limbs assessment.
Lower Limbs Assessment
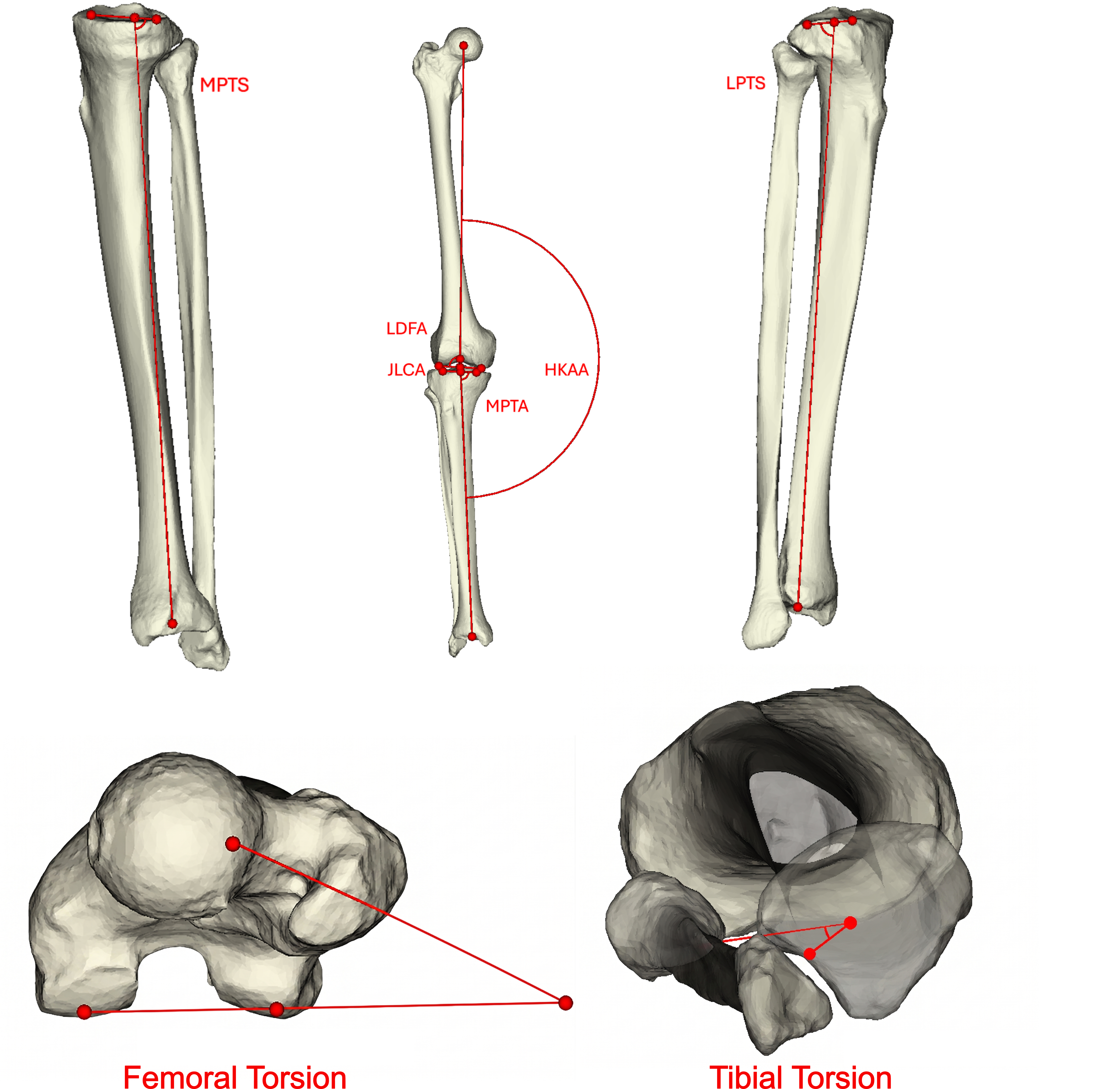
X-ray analysis is used to measure limb deformities in the coronal plane by identifying characteristic angles such as HKAA, LDFA, MPTA, and JLCA. Through 3D reconstruction, it is also possible to assess sagittal (MPTS, LPTS) and axial parameters (femoral and tibial torsion). These angles rely on specific anatomical landmarks that must be easily and consistently identifiable. The development of this system involved the analysis of 3D models derived from the manual segmentation of pre-operative CT scans. Utilizing an expert-validated protocol, 14 specific anatomical landmarks were identified to serve as the essential foundation for calculating characteristic alignment angles. The data collected through this process serves as the basis for 3D reconstruction and automated landmark identification.
3D Reconstruction
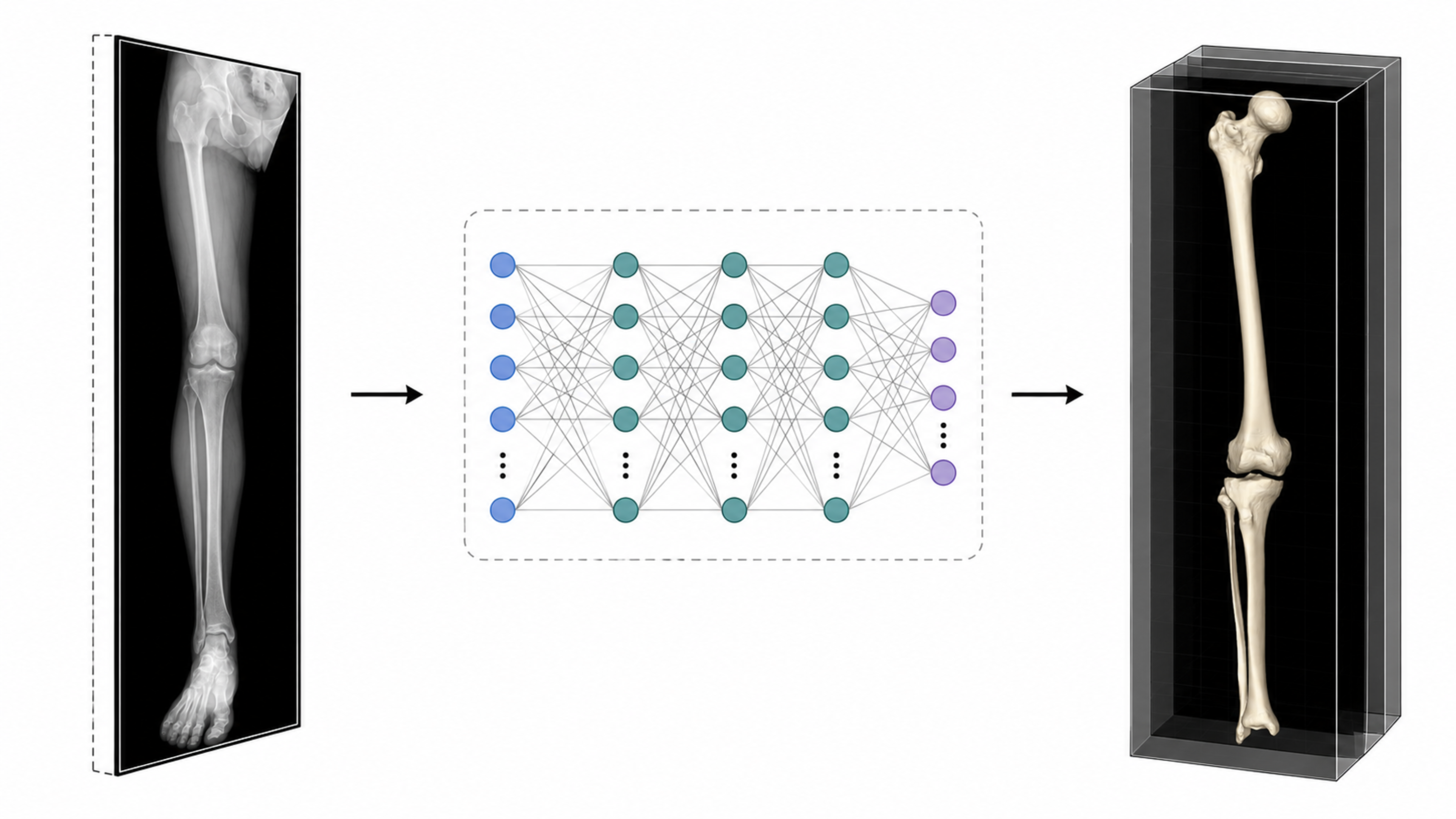
Since 3D imaging modalities, such as CT scans, are not always available in HTO, the first step in the surgical planning process is to generate a patient-specific 3D anatomical model. This model is reconstructed from conventional 2D X-ray images by fitting a statistical shape model that captures the variability of the underlying anatomy. In particular, neural implicit representations are trained using a neural network to generate a continuous 3D representation of the anatomical structure. The resulting model is particularly suitable for the project because it can be manipulated in 3D, enabling operations such as articulation, alignment analysis, and virtual cutting.
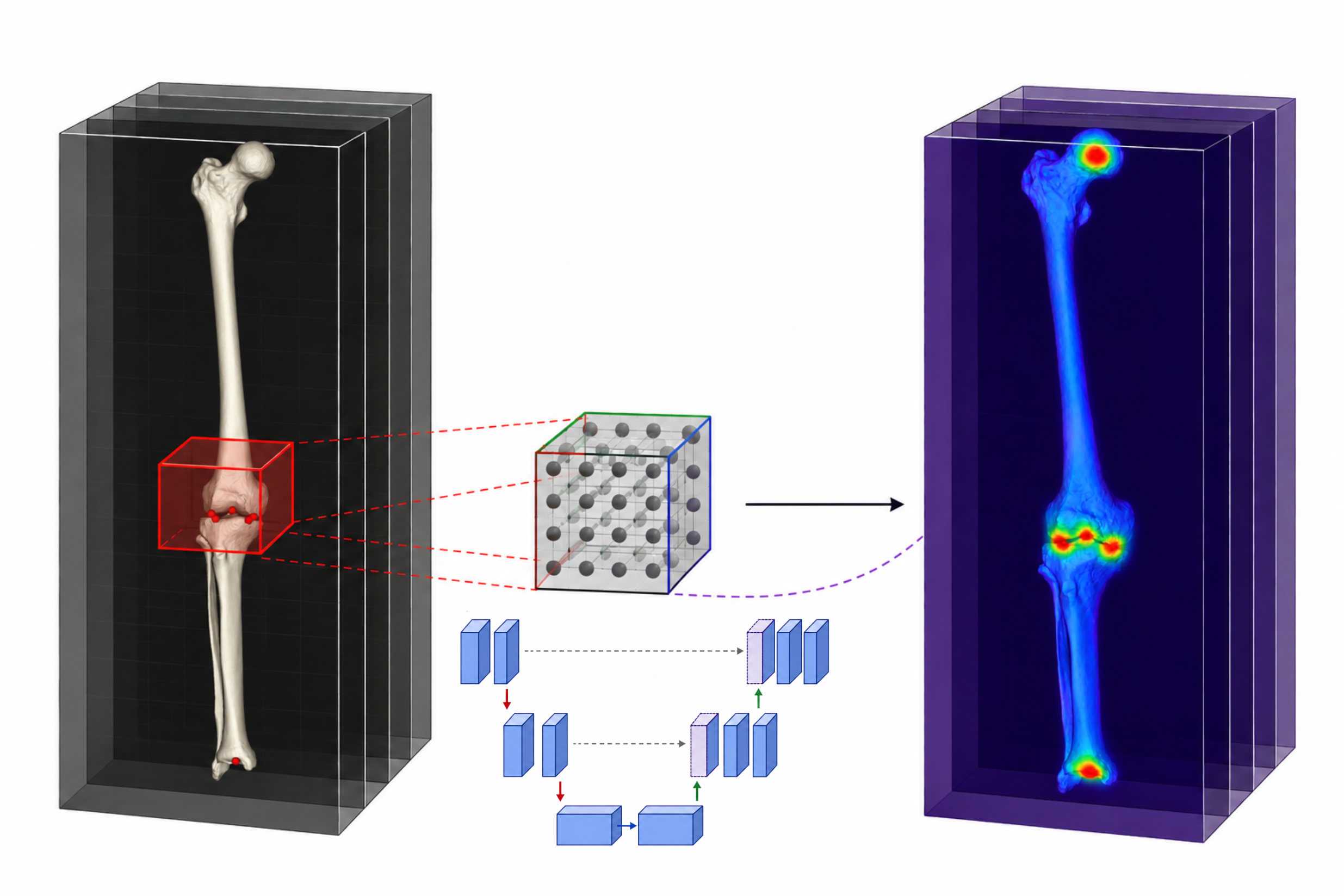
Automated Landmarks Detection
To measure the previously defined angles, the corresponding anatomical landmarks must be identified, as these points form the basis for determining the correction angle. In current clinical workflows, the correction angles are manually determined by medical experts, making the process time-consuming, costly, and dependent on specialized human effort. To automate this step, a neural network is trained using a heatmap regression approach to predict the anatomical landmarks for a given anatomy. Based on these predictions, the relevant angles can then be computed automatically, significantly reducing the need for manual expert intervention.
Planning
The planning process involves a digital simulation of the osteotomy, allowing for the precise definition of the tibial opening or closing wedge. By leveraging 3D reconstruction and multi-planar assessments, this approach goes beyond standard coronal correction; it is designed to prevent unintended alignment shifts in other planes and potentially enables the correction of sagittal or axial minor deformities within a single procedure. Furthermore, the simulation evaluates how kinetic parameters, such as the Knee Adduction Moment (KAM), may shift post-operatively. By integrating this static bone simulation with kinetic insights, the objective is to achieve optimal load distribution across the knee compartments.
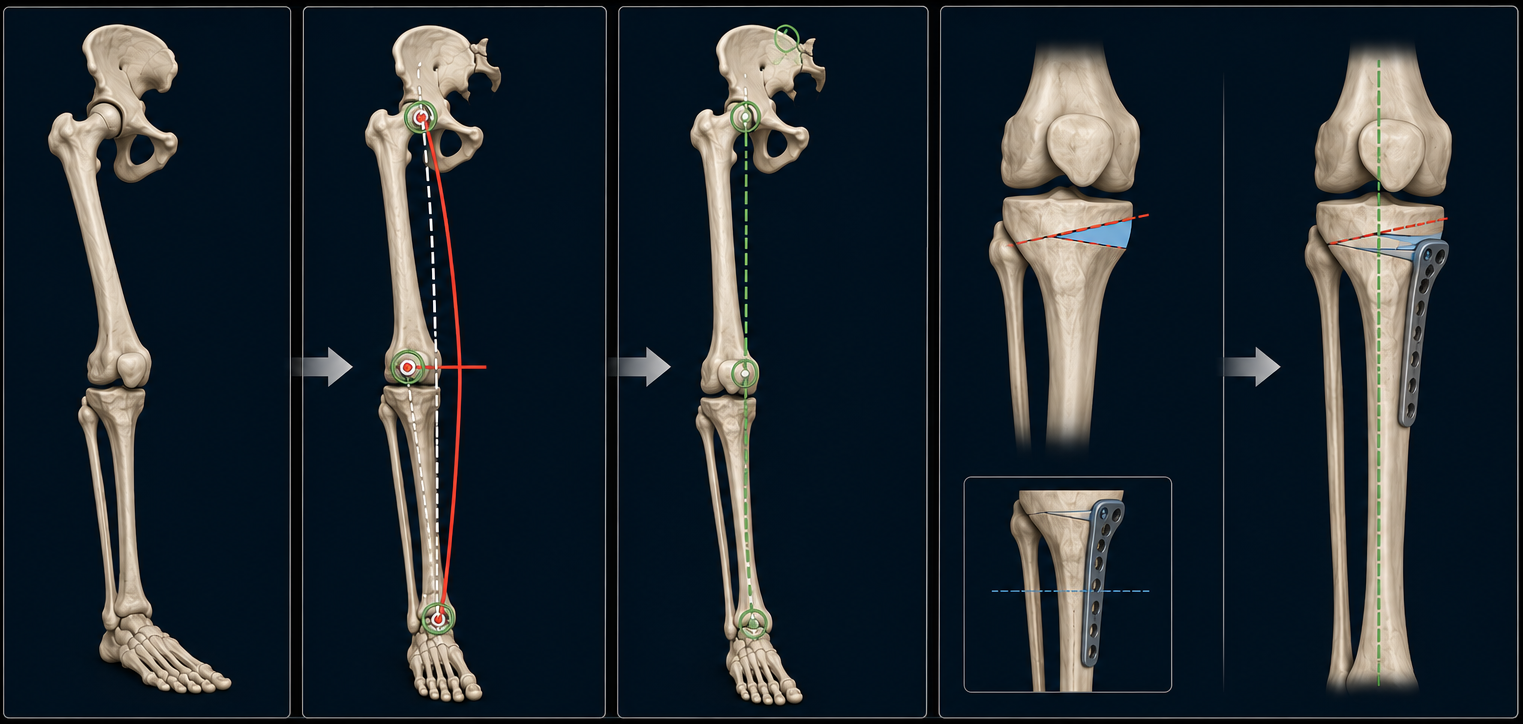
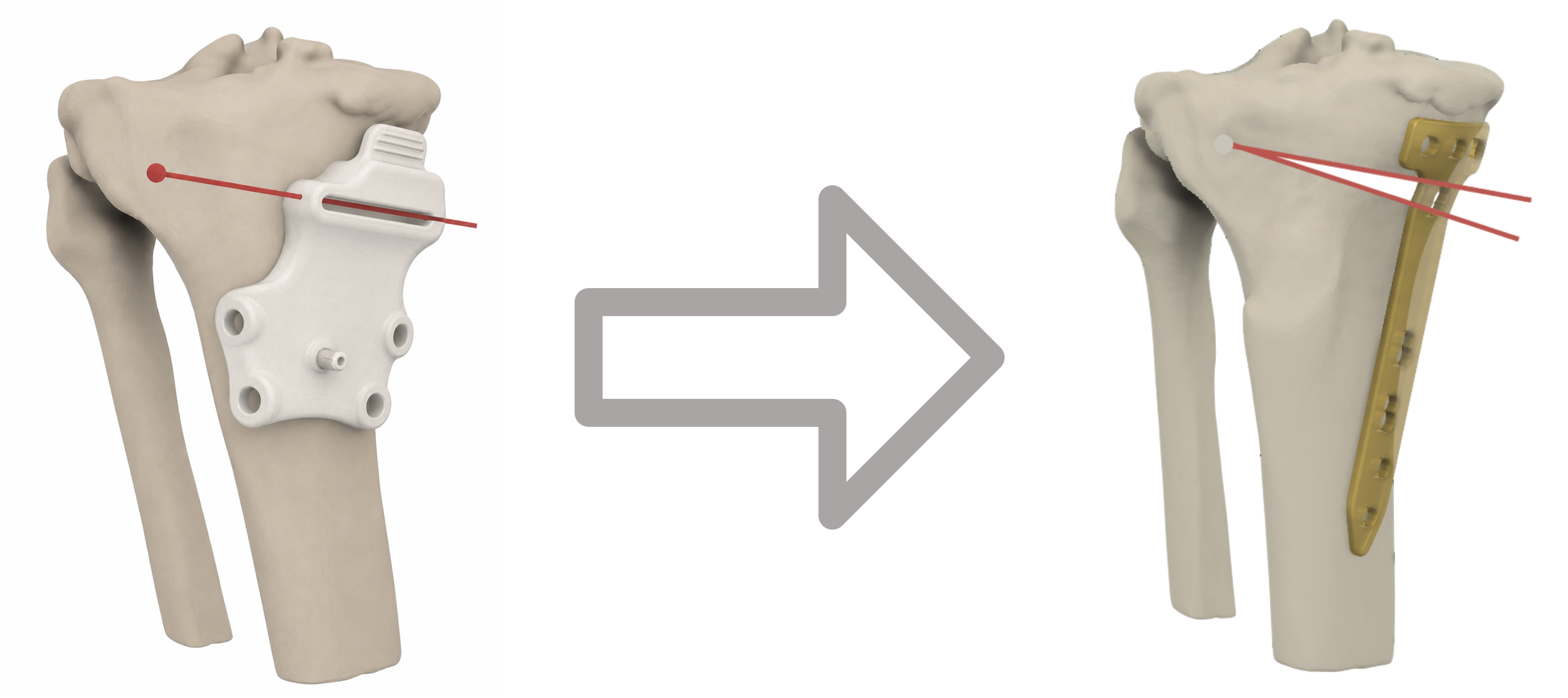
Patient Specific Cutting Guides
Finally, to bridge the gap between digital planning and surgical execution, the process investigates the feasibility of the automated generation of patient-specific cutting guides. 3D reconstruction is intended to provide an anatomical fit of the guide onto the patient’s bone. The planning phase aims to identify the precise target cutting plane, and guides may be produced via additive manufacturing to potentially allow surgeons to operate with enhanced speed and accuracy, aiming for a final result that matches the pre-operative plan.